Hexa-acylated Lipopolysaccharide: How this key metabolite plays a role in inflammation
Author: Anita Tait
March 2021

Could the gut microbiome play a part in inflammation?
Research linking the gut microbiome with diet and disease has come a long way in the last decade. This scientific evidence is currently in a new era with advancements in technology allowing us to accurately measure the abundance and amount of microorganisms as well as their genetic potential to reveal the functions of the gut microbiome. We know the microbes living in our gut produce thousands of compounds called metabolites which act systemically throughout the entire body in ways that can be detrimental or beneficial to health.
Hexa- acylated lipopolysaccharide (hexa-LPS) is one of these metabolites which has been shown to trigger immune activation and systemic inflammation. High levels of hexa-LPS in the blood have been observed in individuals with metabolic and inflammatory conditions such as obesity, heart disease, type 2 diabetes, non-alcoholic fatty liver disease and Alzheimer’s Disease1.
How does our gut microbiome produce Hexa-LPS?
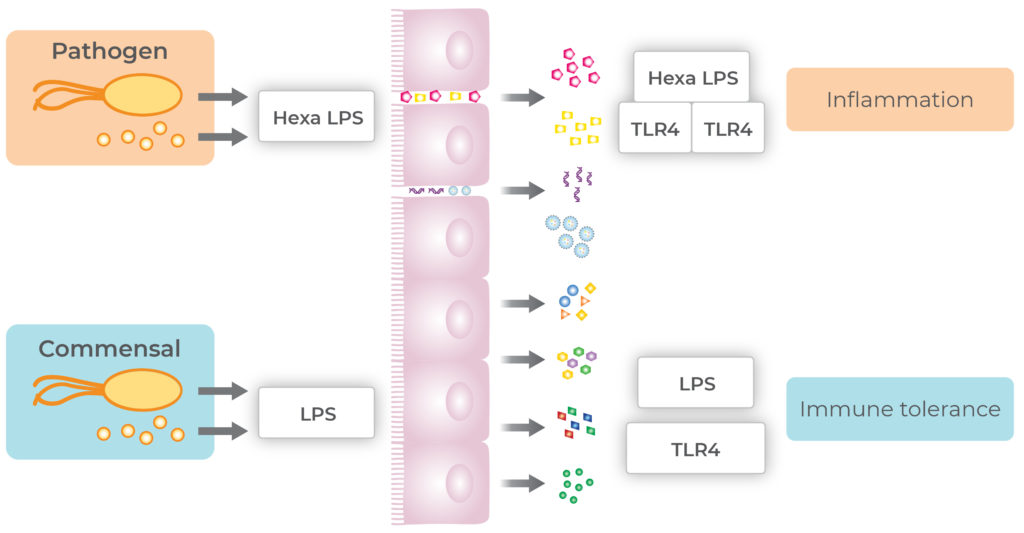
Each bacterial species has its own unique LPS (lipopolysaccharide) signature located within the cell wall. LPS, also known as an endotoxin, is recognised by toll-like receptors (TLR) on immune cells with the lipid A component of LPS being the most important component in terms of interaction with the immune system2. Most species of bacteria within the Proteobacteria phylum produce lipid A with 6 (hexa) or 7 (hepta) fatty acids acyl chains which have strong immunostimulatory power2.
To identify pathogenic bacteria immune cells have a TLR4/MD-2 complex that binds to the lipid component of LPS2. If the LPS has 6 or more acyl chains (hexa-acylated) the sixth acyl chain interacts with a second TLR4 triggering activation of the inflammatory cascade resulting in the generation of pro-inflammatory cytokines2.
Inversely, our commensal bacteria contain different LPS signatures, which often contain 5 or less fatty acid acyl chains. Without this 6th fatty acid acyl chain the TLR4/MD-2 complex does not trigger the inflammatory cascade resulting in immune tolerance. This is how our immune system learns to live in harmony with our commensal and good bacteria while reacting to pathogens.
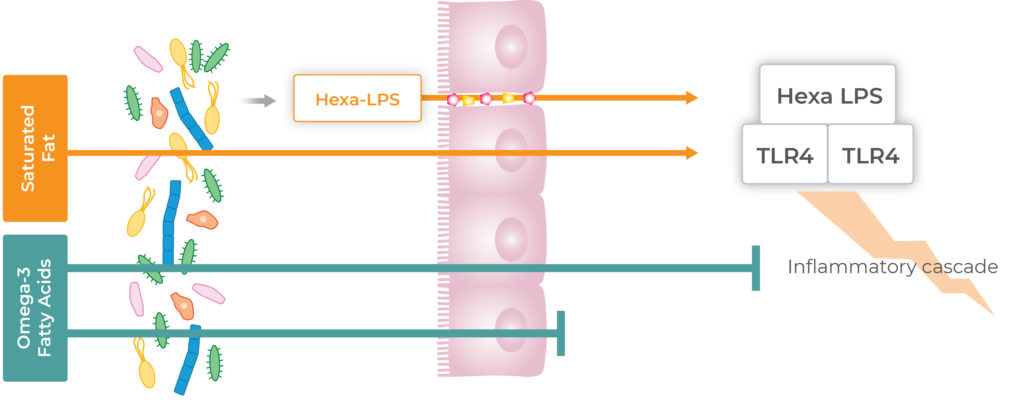
It is important to consider that hexa-acylated LPS isn’t a problem until it crosses the gut barrier to interact with the immune system in the systemic circulation. In particular, saturated fat has been shown to help LPS cross the intestinal barrier and enter the bloodstream3. Research shows that saturated fat increases postprandial blood LPS levels while omega-3 fatty acids decrease postprandial blood LPS levels3. This is where diet can play an integral role in terms of clinical interventions when the potential for the gut microbiome to produce hexa-LPS is shown to be higher than the optimal range.
The Insight gut microbiome analysis identifies individuals whose microbiomes have a high potential to produce hexa-LPS which allows for targeted dietary interventions for patients at risk of or with existing inflammatory conditions.
What dietary interventions can reduce hexa-LPS production?
If the microbial potential to produce hexa-LPS is found to be sitting in the high range within an Insight gut microbiome analysis result, personalised dietary recommendations include limiting saturated fat intake and maximising omega-3 fatty acid and fibre intake. These recommendations also align with Mediterranean dietary patterns which are backed up by an abundance of long-standing scientific research highlighting the links to positive health outcomes8,9.
Limiting saturated fat
Limiting saturated fat in clinical practice is commonplace when it comes to recommendations for a healthy diet and reducing the risk of Cardiovascular Disease. Therefore, these interventions are not necessarily a new concept for many Healthcare Practitioners, however, targeting this intervention based on the gut microbiome can maximise effectiveness.
Avoiding excessive intake of saturated fat can help reduce the ability of hexa-LPS to enter the bloodstream3. Reducing saturated fat within the diet can be achieved through the reduction of foods such as processed meats, butter, high-fat dairy (ice-cream), ultra-processed snack foods (biscuits, cakes chocolate), coconut oil and tropical oil-based products. The Suggested Dietary Target for saturated and trans-fat recommends limiting intake to less than 10% of total daily energy intake7.
Increasing omega-3 fatty acids
Inversely, increasing omega-3 fatty acids to optimal levels through long term dietary patterns rich in fish has been shown to be associated with lower plasma LPS levels4. The three main omega-3 fatty acids that have been shown to have anti-inflammatory properties include alpha-linolenic acid (ALA), eicosapentaenoic acid (EPA), and docosahexaenoic acid (DHA). Increasing dietary sources of omega-3 fatty acids can include foods such as oily fish (canned sardines or salmon) and for those individuals on a vegan or vegetarian diet flaxseeds, flaxseed and canola oil, chia, walnuts, soybean and soy products. Algae supplements can also be an excellent way of increasing EPA and DHA types of omega 3 fatty acid for those who do not eat fish.
The Heart Foundation provides useful guidelines for the recommended amount of omega-3 fatty acids which suggest consuming 250-500mg of EPA/DHA per day (2-3 serves of oil fish per week) and 1 gram of ALA per day (1 teaspoon of flaxseed oil or 3 teaspoons of flaxseeds)5.
Another dietary intervention to consider includes increasing fibre intake from a range of fruits, vegetables and wholegrains. Research shows that increasing fibre intake protects the gut barrier which prevents LPS from crossing the gut barrier and reduces inflammation. A dietary intervention study showed that consuming 3 serves of fruit and vegetables or 3 serves of wholegrains per day resulted in a reduction in the marker of LPS and inflammation in the blood6.
In addition, we have a growing body of evidence that suggests that the metabolites butyrate and 3-indolepropionic acid (IPA) are associated with an improved gut barrier function. Studies have indicated that consuming foods high in dietary fibre, and in particular rye (found in bread, pumpernickel, cereals, crackers) can help increase IPA production10. While consuming foods high in resistant starch11 (found in lentils, peas, beans, cooked and cooled potatoes, rolled oats) have been shown to increase butyrate levels.
Summary
Research confirming the link between the gut microbiome and disease is allowing us to broaden the scope of clinical conditions that are associated with the gut microbiome. We can now broaden our thinking to investigate the function of the gut microbiome for not only those patients with gut symptoms but for those that have an existing chronic disease and those that may be at risk of developing inflammatory or metabolic conditions.
In particular, gut microbiome analysis can measure the genetic potential for the production of hexa-LPS which we know has a central role to play in immune activation and systemic inflammation as well as a range of different metabolic and inflammatory conditions. Dietary interventions such as increasing omega-3 fatty acids, decreasing saturated fat and increasing prebiotic fibre can help to reduce LPS blood levels, reduce inflammation and keep our precious gut barrier healthy.
Insight into the gut microbiome to bring about more detailed and more personalised dietary interventions just may be what individuals need as a key motivator for behaviour change which we know is the key to the kingdom when it comes to creating positive health outcomes.
Find more exclusive practitioner resources on the clinical resources page.
About the author

Anita Tait
Anita is an Accredited Practicing Dietitian, Pharmacologist and Lead Microbiome Coach at Microba with experience in the medical and private practice space. Anita has always been fascinated with human physiology, food and biochemistry, and is now delving into the exciting world of the gut microbiome.
References:
1.Cani, P., Bibiloni, R., Knauf, C., Waget, A., Neyrinck, A., Delzenne, N. & Burcelin, Changes in gut microbiota control metabolic endotoxemia-induced inflammation in high-fat diet-induced obesity and diabetes in mice. Diabetes. 2008;1470-1481. doi: 10.2337/db07-1403.
2.Di Lorenzo, F., De Castro, C., Silipo, A. & Molinaro, A. Lipopolysaccharide structures of gram-negative populations in the gut microbiota and effects on host interactions. FEMS Microbiol Reviews. 2019;257-272. doi: 10.1093/femsre/fuz002
3.Lyte, J., Gabler, N. & Hollis, J. Postprandial serum endotoxin in healthy humans is modulated by dietary fat in a randomized, controlled, cross-over study. Lipids in Health and Disease. 2016;186. doi: 10.1186/s12944-016-0357-6.
4.Ahola, A., Lassenius, M., Forsblom, C., Harjutsalo, V., Lehto, M. & Groop, P. Dietary patterns reflecting healthy food choices are associated with lower serum LPS activity. Scientific Reports, 2017. https://doi.org/10.1038/s41598-017-06885-7
5.The Heart Foundation. 2015. https://www.heartfoundation.org.au/getmedia/4adbe011-db9a-4777-8a99-db6365e27cb1/Consumer_QA_Fish_Omega3_Cardiovascular_Health.pdf
6.Kopf, J., Suhr, M., Clarke, J., Eyun, S., Riethoven, J., Ramer-Tait, A. & Rose, D. Role of whole grains versus fruits and vegetables in reducing subclinical inflammation and promoting gastrointestinal health in individuals affected by overweight and obesity: a randomized controlled trial. Nutrition Journal. 2018;72. doi: 10.1186/s12937-018-0381-7.
7.National Health and Medical Research Council, Australian Government Department of Health and Ageing, New Zealand Ministry of Health. Nutrient Reference Values for Australia and New Zealand. Canberra: National Health and Medical Research Council; 2006.
8.Ghosh, T., Rampelli, S., Jeffery, I., Santoro, A., Neto, M., Capri, M., Giampieri, E., Jennings, A., Candela, M., Turroni, S., Zoetendal, E., Hermes, G., Elodie, C., Meunier, N., Brugere, C., Pujos-Guillot, E., Berendsen, A., De Groot, L., Feskins, E., … O’Toole, P. Mediterranean diet intervention alters the gut microbiome in older people reducing frailty and improving health status: The NU-AGE 1-year dietary intervention across five European countries. Gut, 2020;1218-1228. https://doi.org/10.1136/gutjnl-2019-319654
9.Meslier, V., Laiola, M., Roager, H. M., De Filippis, F., Roume, H., Quinquis, B., Giacco, R., Mennella, I., Ferracane, R., Pons, N., Pasolli, E., Rivellese, A., Dragsted, L., Vitaglione, P., Ehrlich, S. & Ercolini, D. Mediterranean diet intervention in overweight and obese subjects lowers plasma cholesterol and causes changes in the gut microbiome and metabolome independently of energy intake. Gut, 2020; 1258-1268. https://doi.org/10.1136/gutjnl-2019-320438
10.De Mello, V., Paananen, J., Lindström, J., Lankinen, M., Shi, L., Kuusisto, J., Pihlajamäki, J., Auriola, S., Lehtonen, M., Rolandsson, O., Bergdahl, I., Nordin, E., Ilanne-Parikka, P., Keinänen-Kiukaanniemi, S., Landberg, R., Eriksson, J., Tuomilehto, J., Hanhineva, K. & Uusitupa, M. Indolepropionic acid and novel lipid metabolites are associated with a lower risk of type 2 diabetes in the Finnish Diabetes Prevention Study. Scientific Reports. 2017;46337. doi: 10.1038/srep46337. PMID: 28397877; PMCID: PMC5387722.
11.Baxter, N., Schmidt, A., Venkataraman, A., Kim, K., Waldron, C. & Schmidt, T. Dynamics of Human Gut Microbiota and Short-Chain Fatty Acids in Response to Dietary Interventions with Three Fermentable Fibers. mBio. 2019;18. doi: 10.1128/mBio.02566-18. PMID: 30696735; PMCID: PMC6355990.